We never gave their nutrition, nor menopause, a thought. It was the 1980s and as a young nurse, I was working on the surgical ward before moving to the ICU. The four-bed rooms were full of middle-aged women waiting for a cholecystectomy (gall bladder removal). “Fair, Fat and Fifty” was the term that the Consultant Surgeon used to describe the profile of women at risk for gallstones.
And the ‘Fair’ may not refer to the colour of the hair, mentioned a Doctor from the Netherlands, who emailed me recently. “Long ago, when I was a medical student, the Professor mentioned that the ‘Fair’ meant the ‘Fairer Sex, i.e. female” he kindly shared.
There was never a shortage of patients. Week after week they would arrive for their surgery. I never imagined that in my early 50s I would become one of these ‘Fair, Fat and Fifty’ high-risk women too.
I was reminded of this memory last week when I attended a presentation on Ultra Processed Foods (UPFs) at the British Society of Lifestyle Medicine conference.
Ultra Processed Foods (UPFs) are industrially formulated, often made to be highly palatable, ready-to-eat food products that are largely or completely derived from substances extracted from whole foods or additives.
These products are typically cheap, readily available, and tend to be energy-dense with poor nutritional quality. Over the past few decades, modern industrialized food systems have enabled large-scale production of UPFs and the rapidly growing displacement of whole foods from contemporary dietary patterns. Currently, UPFs account for over 57% of dietary intake among adults in the United States [Uche-Anya, 2024].
When I take my presentations and in my online Masterclass on Menopause, I often mention that women in their 50s and 60s today, are unique with regard to the fact that we are the first generation of women to move through menopause into post-menopause within the context of the rapidly changing industrial food environment.
Unfortunately, for those of us who have had UPFs and fast-foods over the decades, this is now known to impact inflammatory changes in the liver and gallbladder. There is mounting evidence linking UPF consumption to adverse health outcomes including all-cause mortality, cancer, cardiovascular disease, inflammatory bowel disease, as well as risk factors for gallstone disease such as obesity and metabolic syndrome [Lane et al., BMJ, 2024].
My private coaching group was full of women telling me that they had had a cholecystectomy – removal of their gallbladder.
That’s what has prompted me to talk to you about your ageing gallbladder. Whether you still have a gallbladder or not, then please read on – it’s an important topic, especially for those of you on oestrogen-based hormonal therapy as research suggests that for those on oral oestrogen hormonal therapy, the risk of experiencing gallstones may be higher. (Dhiman & Chawla, 2009; Cabot & Jasinska, 2013; Wang et al., 2017).
Peri-menopause and Menopause are a known risk for Gallbladder problems. So, too is being overweight which increases the risk of getting gallstones by around 80% (Cabot & Jasinska, 2013).
Why is the Gallbladder important?
It’s not so much the gallbladder that’s important – afterall, this is just a storage organ. It’s the bile that it stores that’s important. Bile is a greenish yellow, thick, sticky fluid – most of us know this colour from when we are sick and vomiting.
Bile consists of bile salts, electrolytes (such as sodium and bicarbonate), bile pigments, cholesterol, and other fats (lipids). It has two main functions:
- Bile aids in digestion by making cholesterol, fats, and fat-soluble vitamins easier to absorb from the intestine.
- Bile assists in the elimination of certain waste products (mainly hemoglobin and excess cholesterol) from the body.
Adult humans produce 400 to 800 ml of bile daily but in women as we age, this can change depending on our diet and how much we are fasting – too much fasting causes a decrease in bile production.
About half the bile secreted between your meals flows directly through the common bile duct into the small intestine. The rest of the bile is diverted through the cystic duct into the gallbladder to be stored.
However as we age and move through menopause, there are changes to the diameter of the extrahepatic bile ducts. These are the small vessels/ tubes that carry bile outside of the liver and as we move into post-menopause, like our blood and lymphatic vessels, these bile ducts are losing some of their elasticity. (Bachar et al, 2003).
Up to 90% of the water in bile is absorbed into the bloodstream, making the remaining bile very concentrated. This concentrated bile is stimulated to release into the small intestine, when food enters the small intestine.
A series of hormonal and nerve signals triggers the gallbladder to contract and the sphincter of Oddi to relax and open. Bile then flows from the gallbladder into the small intestine to mix with food contents and perform its digestive functions.
As we age however, this contraction ability can change because of the reduction in elasticity of the extrahepatic bile ducts.
For women entering peri-menopause and going into post-menopause, this means that there is greater risk for bile and cholesterol deposits to sit in the gallbladder for longer – especially if we are mainly sedentary and don’t do a lot of physical activity – movement helps to keep the gallbladder functioning too.
Gallbladder Problems in Menopause and Post-Menopause
Many of us have heard of gallstones and these form in the gallbladder. Gallstones are hard masses consisting mainly of cholesterol and they may form in the gallbladder or bile ducts thus blocking the flow of bile from the gallbladder, causing pain (biliary colic) or inflammation.
Some of you will have experienced gallstones and had a cholecystectomy (removal of gallstones) and some of you may have experienced cholecystitis, which is inflammation of the gallbladder – this is why, if you have pain around your liver and gallbladder region, then get it checked out with your Doctor.
Gallstones form when bile stored in the gallbladder, hardens into stone-like objects. “This process can take years” mentions Australia’s Dr Sandra Cabot, a reknowned liver health Physician.
One of the main issues with gallstone formation, relates to high amounts of cholesterol and fats in our diet, as well as a higher intake of ultra processed foods, including sweeteners and additives.
If the concentration of cholesterol in the bile becomes too high, relative to bile acids (which help to break down cholesterol) cholesterol can precipitate out and form stones. As those of you who have had gallstones know, if they get stuck in a duct, the pain can be excruciating … remnants of my nursing memories seeing women in tears with the pain, remind me of this!
Other conditions include a thickening of bile (this is a precursor to gallstones); gallbladder polyps (nodules) or a thickening of the wall of the gallbladder. Again, all conditions that need an ultrasound test, so please check in with your Doctor.
Gallbladder conditions are incredibly common and have been for years based on my experience in the surgical wards back in the 1980s!
But what we have to remember however, is that gallbladder problems are first and foremost a digestive and liver problem, hence, another reason to change our diet up a bit during menopause – especially if we are overweight, as I was too.

Preventing the risk of Gallstones in Menopause
Whilst I have a PDF handout for women on my programmes who have had a cholecystectomy (gallbladder removal) over the years, here are some key tips for you to consider as you help your gallbladder to move through menopause with you.
For over 40 years, the Nurses Health Study in America , has generated data that helps us understand how to look after ourselves as we age. One of the findings has been about how much cholesterol (as well as protein), may contribute to increased risk of gallstones. (Tsai et al, 2004)
Cholesterol and its derivatives are important constituents of cell membranes and precursors of other steroid compounds, but too much cholesterol isn’t a good thing. A high proportion of low-density lipoprotein (LDL-Cholesterol) in the blood is associated with an increased risk of coronary heart disease and is also known to contribute to higher amounts of cholesterol deposits in bile.
For women at risk (those overweight), higher amounts of cholesterol in bile, can contribute to gallstones.
That’s why, despite the encouragement to eat saturated fats from eggs, meat and dairy in both the Keto and Paleo diets, we need to watch the amounts of saturated fats as we move through menopause. I talk about this in all of the MyMT™ programmes.
De-cluttering your Gallbladder in the Prevention of Gallstones
Even though your body needs some cholesterol to maintain your health, the problem is when we have large amounts of it being produced in our liver. Don’t get me wrong, cholesterol production is important and your liver and intestines make about 80% of the cholesterol you need to stay healthy.
About 20% comes from the foods you eat, so as we move through menopause, we do need to be cautious about how much cholesterol is formed in our body, because for too many women, higher cholesterol formation may lead to gallstones.
So, it makes sense to follow some of the best advice for looking after our gallbladder and bile production, and this is to:
- Keep the bile flowing and to prevent bile sludge.
- Eat healthy Omega 3 fats (plant-based). A common misunderstanding is to go low fat, but if your fat intake is too low, then you won’t absorb the fat-soluble vitamins very well. Vitamin D is one of these, and this is essential to get enough of during our menopause transition.
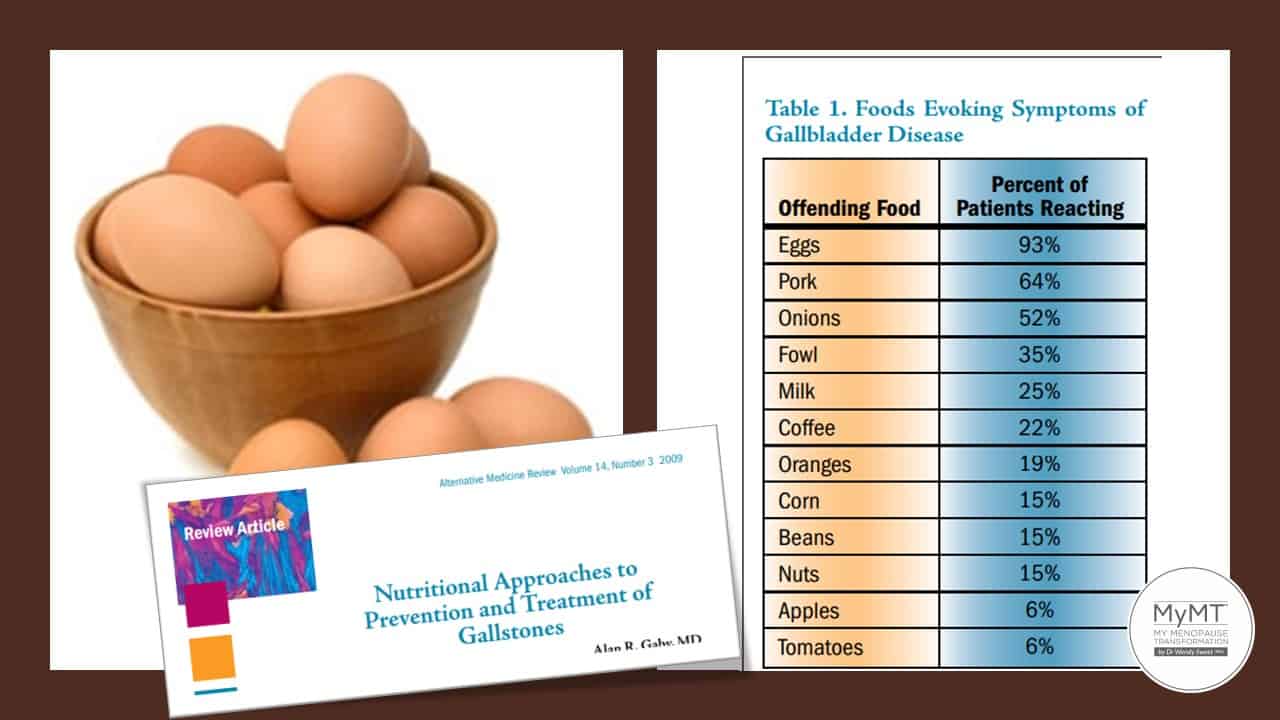
- Reduce your higher-cholesterol foods – e.g. eat fewer eggs (1 a day is fine), red meats and whole-fat dairy products. Too much pork or bacon may be a culprit too. (Gaby, 2009).
- Reduce refined sugar processed carbohydrates and omega-6 rich vegetable oils, e.g. margarine and soybean oil (DiNicolantonio & O’Keefe, 2018) which may also contribute to becoming overweight, which in turn contributes to gallstone risk.
- Increase foods that help to increase bile production and secretion. These foods tend to be bitter foods according to Dr Cabot – Beet leaves, Dandelion leaves, Chicory Leaves to name a few. St Mary’s Thistle is also a good herb for the gallbladder.
- Do some vegetable juicing.
- Avoid constipation
- Get any digestion issues checked with your Doctor – one of the more common ones in menopause which may be related to gallbladder problems is known as GERD or Gastro-oesophageal Reflux Disorder.
- Be careful with oestrogen hormone therapies (Dhiman & Chawla, 2006; Wang, 2017)
- Get support to lose weight if you are overweight – visit MyMT™ Transform Me
- Try not to do too much fasting – a regular food intake helps to improve and move bile flowing through your gallbladder into your small intestine.
- Undertake rhythmic aerobic exercise daily.
As I often say, menopause and post-menopause can be a vulnerable time for changing health and our liver and gallbladder health is no exception. Even if you’ve already had a cholecystectomy, the above principles apply to you as well.
Dr Wendy Sweet (PhD)/MyMT™ Founder and Member: Australasian Society of Lifestyle Medicine

References:
Bachar GN, Cohen M, Belenky A, Atar E, Gideon S. (2003). Effect of aging on the adult extrahepatic bile duct: a sonographic study. J Ultrasound Med. Sep;22(9):879-82.
Cabot, S. & Jasinska, M. (2013). Save your gallbladder and what to do if you’ve already lost it. Phoenix, USA: International Inc Publ.
Dhiman RK, Chawla YK. (2006). Is there a link between oestrogen therapy and gallbladder disease? Expert Opin Drug Saf. 5(1):117-29. doi: 10.1517/14740338.5.1.117. PMID: 16370961.
DiNicolantonio JJ, O’Keefe JH. (2018). Omega-6 vegetable oils as a driver of coronary heart disease: the oxidized linoleic acid hypothesis. Open Heart 5:e000898. doi: 10.1136/openhrt-2018-000898
Gerber LH, Weinstein AA, Mehta R, Younossi ZM. Importance of fatigue and its measurement in chronic liver disease. World J Gastroenterol. 2019 Jul 28;25(28):3669-3683.
Harvard Medical School (2019). How it’s made: Cholesterol production in your body. Harvard Health Publishing, Online access.
Lane MM, Gamage E, Du S, Ashtree DN, McGuinness AJ, Gauci S, Baker P, Lawrence M, Rebholz CM, Srour B, Touvier M, Jacka FN, O’Neil A, Segasby T, Marx W. Ultra-processed food exposure and adverse health outcomes: umbrella review of epidemiological meta-analyses. BMJ. 2024 Feb 28;384:e077310. doi: 10.1136/bmj-2023-077310. PMID: 38418082
Liang KW, Huang HH, Wang L, Lu WY, Chou YH, Tantoh DM, Nfor ON, Chiu NY, Tyan YS, Liaw YP. (2021). Risk of gallstones based on ABCG8 rs11887534 single nucleotide polymorphism among Taiwanese men and women. BMC Gastroenterol. 14;21(1):468.
Marciani L, Cox EF, Hoad CL, Totman JJ, Costigan C, Singh G, Shepherd V, Chalkley L, Robinson M, Ison R, Gowland PA, Spiller RC. Effects of various food ingredients on gall bladder emptying. Eur J Clin Nutr. 2013 Nov;67(11):1182-7. doi: 10.1038/ejcn.2013.168. Epub 2013 Sep 18.
Tsai CJ, Leitzmann MF, Willett WC, Giovannucci EL. (2004). Dietary protein and the risk of cholecystectomy in a cohort of US women: the Nurses’ Health Study. Am J Epidemiol. 160(1):11-8.
Wang, S., Wang, Y., Xu, J., & Chen, Y. (2017). Is the oral contraceptive or hormone replacement therapy a risk factor for cholelithiasis: A systematic review and meta-analysis. Medicine, 96(14), e6556. https://doi.org/10.1097/MD.0000000000006556
Uche-Anya, E., Ha, J., Khandpur, N., … Chan, A. (2024). Ultraprocessed food consumption and risk of gallstone disease: analysis of 3 prospective cohorts,
The American Journal of Clinical Nutrition, Volume 120, Issue 3, 499-506, ISSN 0002-9165

