One of my goals for those of you who are Health Practitioners, Coaches and Exercise Specialists, working with midlife women, is to encourage you to take a broader perspective on your client’s menopause symptoms, especially when it comes to understanding menopause weight gain.
As such, the consideration of the interaction of the hormonal changes in menopause with lifestyle behaviours, is important.
One of the perspectives that has come to my attention over the years, especially with my own challenges with changing moods during menopause, was exploring the link between menopause-related depression, stress-eating and weight gain.
I wonder if you’ve noticed this with your midlife clients who may be struggling with mood swings and menopause weight gain?
While exploring studies on weight gain in menopausal women recently, I was reminded of menopause-related depression. Nearly 80% of 500,000+ women between the ages of 45 and 65 years, who have completed my menopause symptoms quiz over the past decade, mention that they have experienced menopause weight gain.
That’s why the article from Schrieber and Dautovich fascinated me. The researchers called the menopause transition a “window of vulnerability” for the development of depressive symptoms given the changes in hormonal levels (Schreiber & Dautovich, 2017) and due to feeling depressed, women may run the risk of over-eating in order to ‘cope’.
Sound familiar?
Psycho-social factors such as ‘stress-eating’ play an important role in the association between depressive symptoms and weight, state Schrieber and Dotavich (2017) in their research on menopause-related depressive symptoms and weight gain.
The results highlight the need to focus on both behavioural factors as well as menopausal status when working to resolve menopause symptoms, including weight gain. Understanding this connection is important – as it was for me as well.

Feeling depressed or experiencing frequent mood swings in peri-menopause and menopause is all about the connection between all of the hormones through the HPA-Thyroid Axis, not just oestrogen, progesterone and serotonin. I talk about this in the 12 week CPD Health Practitioner Course.
When reproductive hormones decline during the menopause transition, this impacts other important hormones as well, including serotonin.
Serotonin is one of the main hormones that impact memory, cognition and moods in midlife women. Several lines of evidence suggest that oestrogen may produce its effects on cognition and mood through modulation of serotonergic function (Epperson et al, 2012). Hence, the decline in oestrogen production may affect levels of serotonin in the brain.
Other factors also impact serotonin production, including lack of sleep, inadequate intake of tryptophan, poor gut health (also related to tryptophan absorption) and stress. All factors which impact menopause-depression and for many women, stress-eating.
But there is one other point to make too and that is that Menopause depression is linked to inflammatory changes as well. [Jacka et al, 2018; Mattina et al, 2019]
Inflammation arrives in mid-life, not only due to changes to hormonal production of oestrogen and progesterone, but also as cells and tissues throughout the body change, especially if women have a stressful lifestyle and aren’t sleeping. The role of ‘inflammaging‘ is something that I share with Practitioners on my Menopause-Coaching programmes.
Inflammation comes from numerous sources, so it’s good to explore what these sources may be for your clients.
For example, when Hot Flushes are more than 5 an hour, the body overheats and becomes inflamed. This inflammation can contribute to an acceleration in the decline of SEROTONIN.
But there’s other factors contributing to menopause depression too.
- High cortisol is linked to depression, so too is insomnia. If your clients aren’t sleeping and/ or feeling stressed, then cortisol production may be remaining high throughout the day. Higher than normal levels throughout the day causes greater inflammation in organs, muscles and blood vessels as women biologically age. The accumulation of high levels of cortisol, can disrupt serotonin production more rapidly during menopause. The result? Increased risk of depression, stress-eating and weight gain.
- The health of the gut and liver matter to menopause-depression. When liver inflammation is present in cells and tissues or if women are putting on belly fat and have poor gut health or eating a high fat diet, then B vitamins may not be absorbed and metabolized very well. B-vitamins are important for managing menopause depression.
- Low Vitamin B6 and B12 increase depressive episodes (Feraj, 2017). This is why for women who want to improve their moods and motivation during menopause, it’s important that they get their Vitamin B12 checked as well as improve the health of the liver and gut. This is important for women who are overweight.
The scientific evidence emerging from research into the gut-brain connection is increasing in relevance for women in their menopause transition.
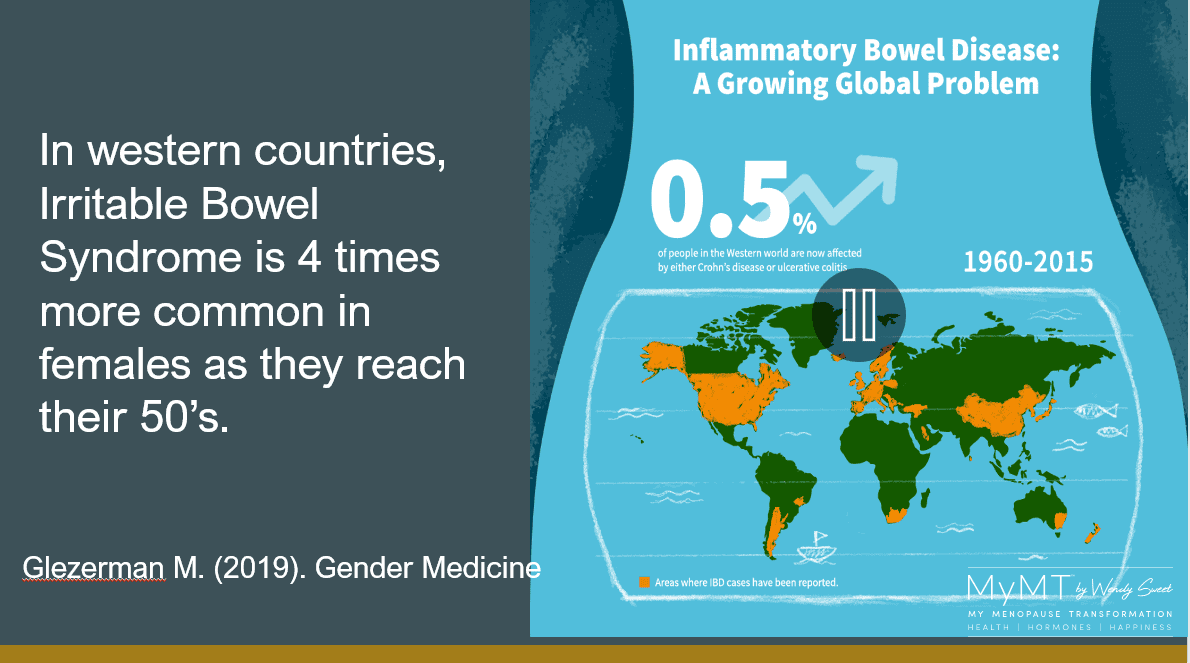
Irritable Bowel Syndrome (IBS) or Diverticulitis is 4 times higher in women during their menopause transition than in other stages of their life. Researchers now understand that the powerful connection between the immune system and the gut microbiome has a profound effect on mental health. This is because gut inflammation impacts on the absorption of a protein called Tryptophan, which helps to make serotonin. [Jenkins et al, 2015]
Helping your Midlife Clients to Reduce Effects of Menopause Depression:
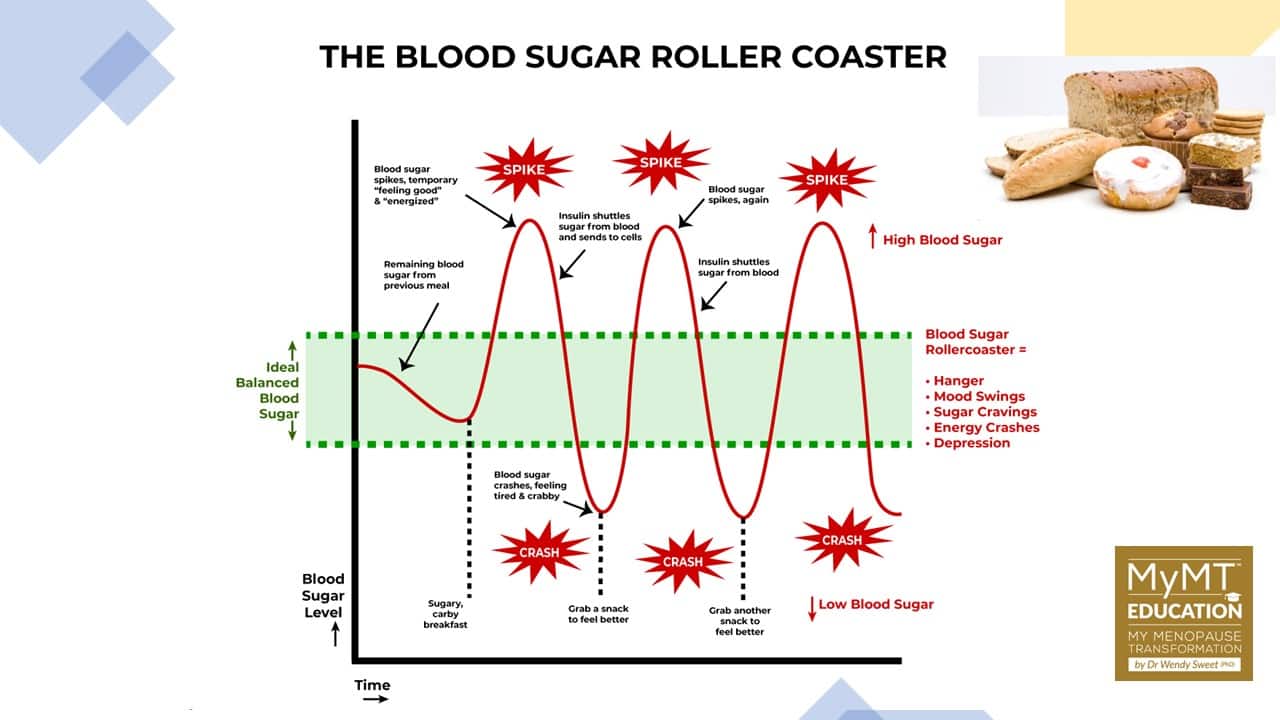
(1) Adjust the type, timing and amount of their food intake. Healthy moods require blood glucose regulation. When women don’t eat regularly or don’t eat the right healthy carbohydrates (especially if they are exercising), this affects insulin production and blood sugar levels.
When blood sugar levels are low, the pancreas secretes a hormone called glucagon to re-set plasma glucose levels. But if women are stress-eating foods which are high glycemic index carbohydrates, then the pancreas releases insulin to help regulate blood sugar levels by moving excess glucose to the brain, liver, and muscles. However, if women are sedentary, this excess glucose may be taken up by fat cells (adipose cells) instead. When both glucagon and insulin are un-balanced, mood swings and feelings of depression may also occur because there is a powerful link between the blood-glucose regulating hormones and serotonin production.
(2) Focus on restoring sleep patterns and reducing hot flush frequency (I discuss this in the Menopause Practitioner Course). Poor sleep means that the adrenal glands (which produce your ‘fight or flight’ hormones), become overwhelmed and this impacts on thyroid function. Low thyroid response results in low energy levels and even more stress on the adrenals. When women are feeling stressed or they have oxidative stress from inflammation in tissues, their sleep generally suffers. As such, hot flushes and mood swings may become worse for them. This is why turning around the circadian rhythm matters more for menopause weight loss in menopause than any crazy diet they may be on!

(3) Vitamin D levels may need to be checked. Especially for those women living in areas where winters are longer, or they spend a lot of time indoors. Low Vitamin D3, depression and worsening inflammation go hand-in-hand. Vitamin D is often low in menopausal women because it decreases with changes to oestrogen receptors in the skin. (Lerchbaum, 2013).
I talk a lot about Vitamin D and this connection with menopause with women, because so many of us work inside and if women have darker skin, then their Vitamin D absorption may be lower too. If women are also overweight and carrying more belly fat, then because Vitamin D is drawn to fat in fat storage areas, the Vitamin D can go to adipose tissue and not to where it is needed – in muscles, bones, nerves and the heart. [Dregan, Rayner, et al., 2020).

In the two to eight year period known as ‘peri-menopause’ the production of oestrogen is declining.
Because oestrogen is a hormone, when levels reduce, this may affect the function of not only progesterone, but other hormones in the body, including the mood hormone, serotonin. When serotonin levels are low, this impacts on other hormones produced by the thyroid, adrenal and more importantly, the pituitary glands where serotonin production occurs.
Depression that arrives during menopause is frightening – especially if women have never experienced it before. Therefore, for those clients who are experiencing this, then they must follow up with their Doctor. You can also help them to explore lifestyle solutions, including the role of stress and stress-eating on weight gain.
No matter whether your clients are on supplements, HRT, bio-identical hormones or medications such as anti-depressants, these lifestyle solutions matter during a stage of their life, whereby managing moods in menopause matters!
Dr Wendy Sweet (PhD)/ Member: Australasian Society of Lifestyle Medicine
References:
Doyne, E. et al. (1983). Aerobic exercise as treatment for depression in women. Behavior Therapy, 14(3), 434 – 440.
Dregan, A., Rayner, L., Davis, K., Bakolis, I., Arias de la Torre, J., Das-Munshi, J., Hatch, S. L., Stewart, R., & Hotopf, M. (2020). Associations Between Depression, Arterial Stiffness, and Metabolic Syndrome Among Adults in the UK Biobank Population Study: A Mediation Analysis. JAMA psychiatry, 77(6), 1–9. Advance online publication.
Epperson CN, Amin Z, Ruparel K, Gur R, Loughead J. Interactive effects of estrogen and serotonin on brain activation during working memory and affective processing in menopausal women. Psychoneuroendocrinology. 2012 Mar;37(3):372-82. doi: 10.1016/j.psyneuen.2011.07.007.
Feraj, J. (2017). Micro-nutrients, depression and inflammation among women of reproductive age. Doctoral Dissertation 993, University of Massachusetts.
Freeman EW. Depression in the menopause transition: risks in the changing hormone milieu as observed in the general population. Womens Midlife Health. 2015 Aug 11;1:2. doi: 10.1186/s40695-015-0002-y.
Jacka FN, O’Neil A, Itsiopoulos C, Opie R, Cotton S, Mohebbi M, Castle D, Dash S, Mihalopoulos C, Chatterton ML, Brazionis L, Dean OM, Hodge A, Berk M. The SMILES trial: an important first step. BMC Med. 2018 Dec 28;16(1):237.
Jenkins TA, Nguyen JC, Polglaze KE, Bertrand PP. Influence of Tryptophan and Serotonin on Mood and Cognition with a Possible Role of the Gut-Brain Axis. Nutrients. 2016 Jan 20;8(1):56. doi: 10.3390/nu8010056.
Lerchbaum, E. (2014). Vitamin D and menopause – A narrative review. Maturitas Journal, 79, 3-7
Mattina GF, Van Lieshout RJ, Steiner M. Inflammation, depression and cardiovascular disease in women: the role of the immune system across critical reproductive events. Ther Adv Cardiovasc Dis. 2019 Jan-Dec;13:1753944719851950.
Schreiber, D, & Dautovich, N. (2017). Depressive symptoms and weight in midlife women: the role of stress eating and menopause status. Menopause (New York, N.Y.), 24(10), 1190–1199.
Scott KA, Melhorn SJ, Sakai RR. Effects of Chronic Social Stress on Obesity. Curr Obes Rep. 2012 Mar;1(1):16-25. doi: 10.1007/s13679-011-0006-3
Vivian-Taylor & Hickey, M. (2014). Menopause and depression: Is there a link? Maturitas Journal, 79, 142-146

